Here is a possible scenario: you can't hear anything when you put the telephone to one of your ears.
Your doctor delivers the bad news — that you have a brain tumor, AND the Good News — that it is perfectly benign.
You are bombarded by different therapy options (Gamma Knife, Surgery, etc.) including the idea to forget about the whole thing.
Everyone and their brother and/or sister have a strong opinion; only you are left to make the decision.
Table of Contents
Welcome To The World of Acoustic Neuromas
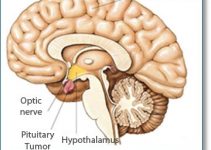
This tumor (called a “schwannoma”) arises from the myelin-forming cells (Schwann cells”) of the 8th cranial nerve at the point where the peripheral part of the nerve meets the brain part of the nerve (called “Hensen's node”).

Hensen's node is usually located in the inner ear canal that leads to our hearing apparatus, called the “acoustic meatus.”
This nerve is actually three nerves in one, two “vestibular” nerves (upon which the tumor actually grows) and the hearing nerve.
Immediately associated with these nerves is the 7th cranial nerve, the nerve that controls the muscles of the face, salivation, tearing, and taste.
The tumor grows just next to the brain stem, and when enlarged may actually compress it.
Larger tumors also may involve the swallowing nerves down below, as well as the 5th nerve above which controls sensation to the face and eye.
In other words, this is a very tightly packed and difficult area for involvement.
Patients may present any combination of symptoms related to malfunction of these nerves, depending on the size, the pressure and location of the tumor.
In patients with an inherited disease called “Neurofibromatosis,” a slightly different type of tumor grows, the “neurofibroma.”
This tumor tends to involve the whole nerve rather than displace a nerve as does the “schwannoma.”
In general, the neurofibroma is somewhat more difficult to handle.
Acoustic Neuromas Tumor Classification

The size determines therapeutic outcome. Therefore, a grading system has been devised to allow both physicians and patients to tailor their expectations for the outcome:
- Grade I – Tumor is small, occurring only within the internal auditory canal itself.
- Grade II – Tumor extends into the fluid spaces around the brainstem
- Grade III – Larger tumor (usually up to 2.5 cm in diameter). It extends up to the brainstem.
- Grade IV – Very large tumor (up to 5 cm in diameter). Compresses the brainstem, often involves the nerves of swallowing and the 5th cranial nerve (face and eye sensation)
Surgical Decisions
Ways to remove the tumor
- Translabrynthine approach. This approach is ideally suited for smaller tumors, especially when all or most of functional hearing is lost in that ear. This approach always sacrifices hearing, so it is not used if there is a chance to preserve hearing.
- Retromastoid approach. This approach is used for small tumors when hearing preservation is a possibility. Saving hearing in these cases is about 50:50. It is also chosen for larger tumors, or for schwannomas that potentially grow from other cranial nerves (e.g. 7th, 5th, 9th ).
- Middle fossa approach. A favored approach by only a few surgeons. Hearing can also be preserved in this way.
Surgical Risks
Cerebrospinal fluid leakage. Surgery in this area may lead to spinal fluid leakage in up to 20% of cases.
This is most often temporary; other procedures may be required to treat this problem if it persists.
The obvious risk of CSF leakage in meningitis requires antibiotic treatment as well.
With today's microsurgical techniques (very small incisions, the use of fibrin glue and new closure techniques) the risk of CSF leakage has been greatly reduced.
7th Nerve Loss. This is the most distressing problem, especially for younger patients. The eye does not close well, tearing is difficult to control, the face droops and friends look at you strangely.
Sensation to the eye might be lost as well, causing abrasions to the cornea.
In cases of large tumors with a thinned out nerve that is splayed over the surface of the tumor, the nerve is physically saved during surgery, but it may only partially recover.
5th Nerve Loss. Loss of sensation to the face and eye is not only disturbing, but it is also potentially dangerous.
The cornea of the eye can be injured when sensation is lost, causing loss of vision.
Swallowing Nerve Loss (9th and 10th nerves). Loss of ability to swallow effectively may lead to aspiration pneumonia when secretions and food travel into the lungs rather than down the esophagus.
Solutions for cranial nerve loss (7th Nerve). It is now possible to effectively reestablish 7th nerve function using a number of methods.
Most of these include reconnection of the nerve with either nerve grafts and/or other nerves (e.g. the opposite of the 7th nerve — the 12th nerve). Other strategies include plastic surgery operations to suspend the face and ophthalmologic placement of a gold weight in the eyelid.
In cases of partial dysfunction of the nerve, electrical stimulation to the face may allow the facial muscles to stay in shape while the nerve repairs itself.
Swallowing Nerves
Problems with swallowing are almost always temporary. Serious loss of swallowing function can be partially repaired via a number of surgical procedures.
In serious cases, a temporary tracheostomy may be needed until swallowing function returns.
Radiation Therapy. Focused beam radiation (e.g. the Gamma knife) has been advocated as a new technology for benign brain tumors, especially acoustic neuromas.

Although tantalizing, and early studies show that acoustic neuromas tend not to grow and may even shrink with this therapy, a few notes of caution are in order:
Historical studies have shown that radiation therapy to the brain and its coverings, even at low dosages, can cause serious problems after a number of years.
One example took place in Israel during the 1950s when children and young adults were treated for a scalp condition called tinea capitis with very low dose radiation therapy (only 1000 Rads).
Over the years (10-30) that followed, many of these people developed meningiomas of the brain. Some even developed malignant astrocytomas.
We also know that patients who survive the usual dosage of radiation to the brain may develop radiation necrosis and in some cases develop malignant brain tumors in the area that was radiated.
Focused beam radiation usually has a dosage of 10,000 -12,000 Rads, enough to give one pause when thinking of long-term results.
Long term results (i.e. greater than 10 years) are still not in.
If a tumor were to continue to grow or recur, future surgery in the area of radiation would be difficult, because of local radiation changes (scarring) to the surrounding tissues and nerves.
Complete surgical removal has been proven to be curative.
The downside of surgery has been markedly reduced, with microsurgical approaches limiting the skull opening to the size of a quarter.
Resources: